A commenter called “Hugh R Delusional”, challenged me thusly:
Can Morgellons watch replicate bundles of colored fibers? If we fiberites are crazy and the fibers we claim to see are simply textile in origin then any doubter should easily be able to pluck some lint off their clothing or belly button even and see bright blue, red, black and translucent fibers tangled in amongst the lint. […]
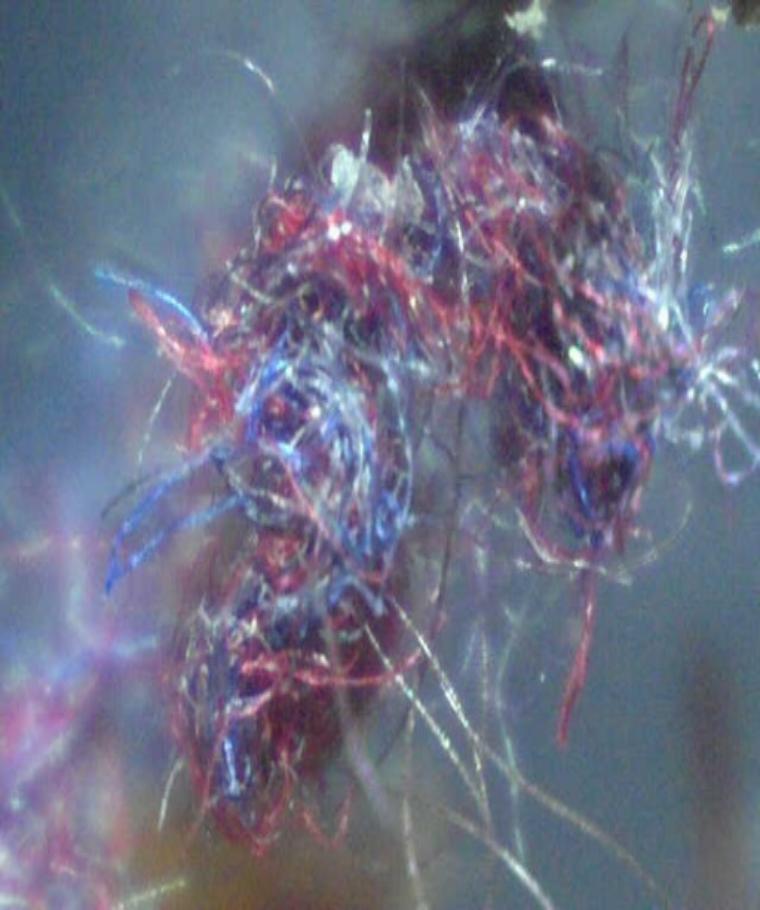
If your curious as to what you should be looking for, go to the main page of morgellonsusa.com and the background picture will give you a clear indication of what to expect.
Here’s the morgellonsusa.com picture:
So I got out my trusty QX5 and scrabbled together a few lint balls from my wardrobe. Unfortunately my microscope only does 10x, 60x, or 200x, so I can’t replicate the scale of the above (which looks 20x), but here’s my best effort at 60x

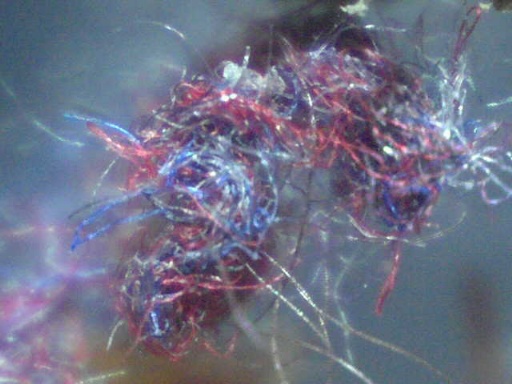
And again at 10x
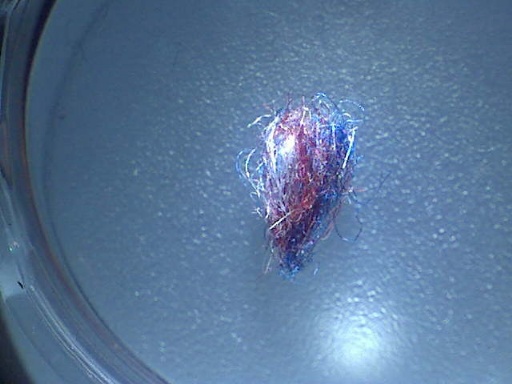
I think that quite conclusively shows that the morgellonsusa fibers are nothing more that regular clothing fibers.
This whole experiment took me less than 20 minutes.
(Update)
Later I discovered that the Morgellonsusa photo was actually squished and elongated, which gives it that odd looking scale. It’s actually a regular 60x QX3/5 photo. Here’s the original:
This is a tiny little thing, barely a spec when viewed at arms length. Easily not noticable on your skin until you look closely. For scale, here’s a bit of MY fuzzball on a penny, at the exact same scale. Note it’s on the letter ‘E’ of ‘CENT’. Also notice how the colors and the fiber diameters all match the morgellonsusa photo.

I also did bit more digging, for Hugh, and found this bit of lint on the floor of the laundry room:

You see, fibers are everywhere. And this bit of lint shows that they are mostly white, with some red and blue, and the occasional black. I think laundry lint is a pretty good random sampling (seeing as I don’t sort my laundry by color).
