There’s a new article on Morgellons by Savely and Stricker – the authors of the original Morgellons paper, and proponents of long-term antibiotics for both late stage Lyme and “Morgellons”
There’s a new article on Morgellons by Savely and Stricker – the authors of the original Morgellons paper, and proponents of long-term antibiotics for both late stage Lyme and “Morgellons”
Expert Review of Dermatology
October 2007, Vol. 2, No. 5, Pages 585-591
Morgellons disease: the mystery unfolds
Virginia R Savely and Raphael B Stricker
http://www.future-drugs.com/doi/abs/10.1586/17469872.2.5.585
Abstract:
Morgellons disease is a mysterious skin disorder that was first described over 300 years ago. The disease is characterized by fiber-like strands extruding from the skin in association with dermatologic and neuropsychiatric signs and symptoms. Although Morgellons disease has been confused with delusional parasitosis, the occurrence of the disease in children, the lack of pre-existing psychopathology in most patients and the presence of subcutaneous fibers on skin biopsy indicate that the disease has a somatic origin. The association with Lyme disease and the apparent response to antibiotic therapy supports the concept that Morgellons disease may be triggered by an infectious process. Recent studies suggest that infection with Agrobacterium may play a role in the disease. Further clinical and molecular research is needed to unlock the mystery of Morgellons disease.
The full article was posted to various Morgellons mailing lists, and is available here:
http://nielsmayer.com/morgellons07.pdf
Overall the paper is very disappointing. There is very little (if anything) in the way of new information. It seems very much a re-working of the old paper, with some additions of various things that have already been mentioned in the popular press. There is no new science. No real studies, and nothing in the way of case studies.
Here I’ll focus on the more obvious (and sometime imponderable) flaws.
The disease was first described in French children in 1674 by a British physician, Sir Thomas Browne
No, it was not. A totally different disease with the same name was described. Browne writes about a local disease of children characterized by coughs and convulsions that is capped by “harsh hairs on the back”. There is nothing to suggest any link, and the MRF does not claim one.
 In 1682, Dr Michel Ettmuller’s microscopic drawings of objects associated with what was then believed to be a worm infestation of children (Figure 1) appear similar to microscopic views of fibers from present-day sufferers of this disease
In 1682, Dr Michel Ettmuller’s microscopic drawings of objects associated with what was then believed to be a worm infestation of children (Figure 1) appear similar to microscopic views of fibers from present-day sufferers of this disease
No, they don’t. Mites E are scabies mites, B is some kind of insect larvae (mosquito maybe) C and D are just some other mites, or perhaps a fuzzball from clothing. Fibers look like fibers, especially 300 years ago. There is no connection here.
Morgellons disease was rediscovered in 2001 by a Pennsylvania housewife, Mary Leitao
Maybe they should have checked with her first. She’s said all along that this was just a label, and nothing to do with the original “Morgellons”.
Morgellons disease was initially considered to be a form of delusional parasitosis (DP) by most dermatologists [3–11]. However, as the disease has become more widely recognized, significant clinical differences from DP have become apparent (as discussed later) [12,13,102]. The recent discovery of a putative infectious cause of the disease supports a somatic etiology of this bizarre skin condition.
Dermatologists options have not changed, and they are not as simple as suggested here. If there is something wrong with a patient’s skin, then it’s not DP. Delusions might play a part, but people can have skin problems, and also have delusions at the same time.
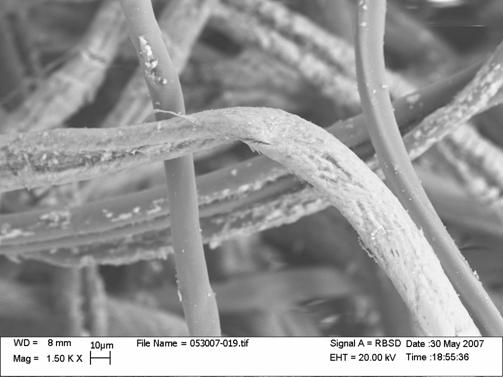
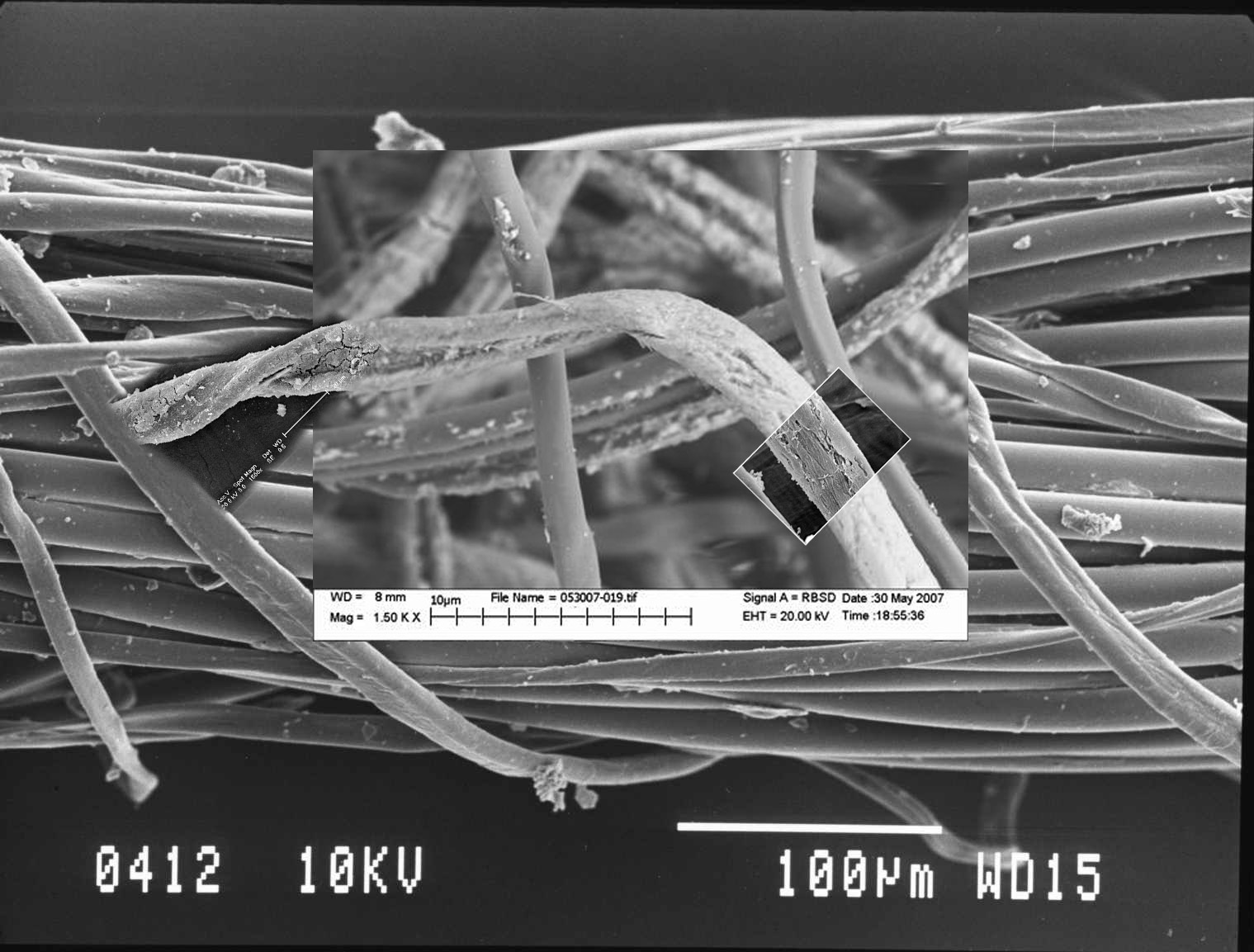
A network of blue, red, white and black fibers under the skin of these patients as well as blue, black and white fibers protruding from the lesions can be visualized using a 30× hand-held digital microscope […] The fiber-like material can be observed in skin lesions as either single strands or what appear to be balls of fibrous material that may demonstrate autofluorescence (Figure 4) [1]. Patients frequently describe this material as ‘fibers’, ‘fiber balls’ or ‘fuzz balls’.
Here note they are trotting out the same descriptions that have been going around for years. Red, white, blue and black fibers on and under the skin, and fuzz balls. This is the crux of the matter here. What could these fibers be? After several years nobody has been able to identify any fibers EXCEPT those fibers which were clothing fibers.
Typically, patients have sought help from 10–40 physicians who often make a diagnosis of DP without a thorough examination and interpret the obvious open sores on the patient’s skin as attempts at self-mutilation
Now this might hold some weight if they had a cohort of patients that they could actually demonstrate had some skin problems that 10-40 doctors had simply dismissed. Unfortunately they are unable to do this. If there are over 10,000 patients, then that’s around 200,000 times that doctors had “dismissed” the lesions as self-inflicted. A better word might be “diagnosed”. 200,000 diagnoses, and all 200,000 wrong? Clearly not. In fact, this large number of similar diagnoses seems to suggest that the diagnoses is correct. If you go to 20 doctors, and they all tell you the same thing, then does this make it more or less likely that your self-diagnosis is correct?
We currently follow more than 200 Morgellons patients in our practice in San Francisco.
So they diagnose Morgellons. And treat it.
The male to female ratio is approximately 1:1 according to the Morgellons Research Foundation. The disease affects all age groups including children, but the prevalence in children is unknown at present. There is often a history of traumatic exposure to plants, dirt or soil, such as gardening, landscaping, farming, camping or other outdoor activities. The association with plant exposure has implications for the etiology of the disease (as discussed later).
This is getting silly. Who has not had “a traumatic exposure to plants, dirt of soil” in the last ten years? Scuffed a knee? Grazed a knuckle? Potted a plant? What was the questionnaire question for this? It’s not mentioned on the MRF survey. What is the sample size?
It appears that skin lesions and fibers may not be present in all individuals with this disease, since family members of patients often report similar systemic symptoms without skin lesions
Brilliant, you don’t even need lesions or fibers to have Morgellons. So what, then, is the case definition for? If you just had the symptoms of Menopause, you would qualify for Morgellons. If you were simply getting old, you could quite easily diagnose yourself with it.
Patients have reported symptoms of this disease in their pets [1]. The majority of reports involve dogs, but cats appear to be increasingly affected. Skin lesions fitting the description of Morgellons disease have also been reported in horses, and horse owners have observed fibers associated with skin lesions on their animals by using a lighted 30× hand-held microscope [1].
What are we to make of this? Dogs and cats? Horses? Reported by the patients? This is getting ludicrous.
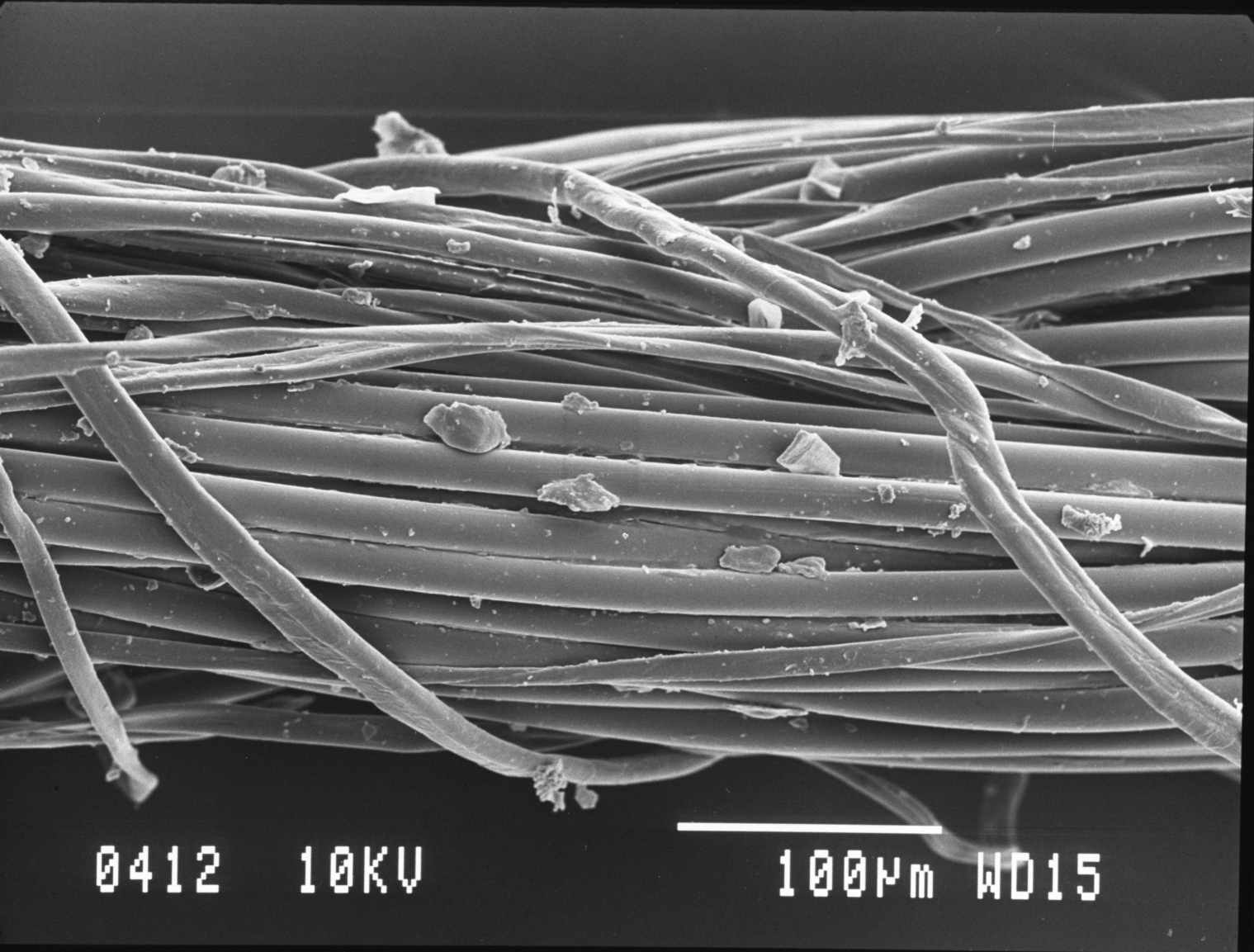
Skin biopsies of patients typically reveal nonspecific pathology, or an inflammatory process with no observable pathogens [1]. Several biopsies have shown fibrous material projecting from inflamed epidermal tissue. Often the biopsies are reported to contain ‘textile fibers’ located in the dermal region rather than being adherent to the skin. How these fibers arrive at a subcutaneous location remains unexplained.
This is called an “argument from ignorance” – we can’t figure out how those fibers got there, so it much be some freaky bacteria! A more sensible approach would be to first question these reports. How many, and from whom? Then you might consider the thousand ways that fibers MIGHT get under unbroken skin. Start with light neurotic excoriations which healed over. Then perhaps consider fibers inside follicles. Anyway, you do the math.
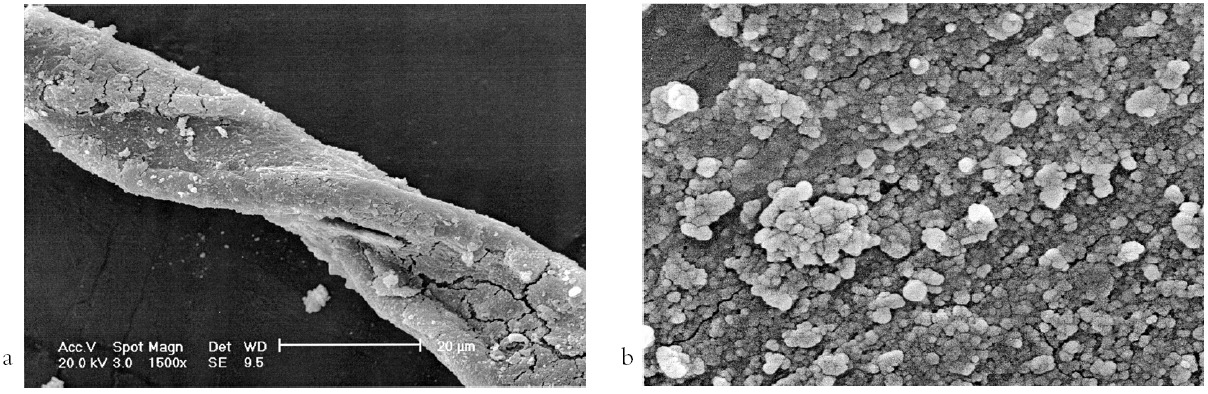
Recent studies indicate that Morgellons fibers are resistant to chemical solubilization and heating, making analysis difficult by conventional means […] There is preliminary information that some Morgellons fibers are made of cellulose, but this information has neither been formally evaluated nor confirmed
So which is it? Resistant to heating, or cellulose? There’s also studies that indicate they are wool and cotton. How do you pick which study to choose? Simply the one the fits your facts best. Better be careful and not pick too many.
In a preliminary study, skin biopsies from Morgellons patients revealed evidence of infection with Agrobacterium, which causes crown gall disease in plants [20]
[20] here is “Stricker RB, Savely VR, Zaltsman A, Citovsky V. Contribution of Agrobacterium to Morgellons disease. J. Invest. Med. 55, S123 (2007). • First description of Agrobacterium in Morgellons patients.” What happened here was Stricker sent Citovsky TWO samples from sick patients with open sores on their skin. Citovsky tested them, and also six samples from health patients with nothing wrong with their skin. The sick patients with skin problems were found to test positive for Agrobacterium. The healthy patients did not.
That’s it. Samples of dubious origin with no appropriate control group, in a statistically meaningless amount. At best it suggests that people who have constant open lesions on their skin due to neurotic excoriations tend to have agrobacterium in the tissue around those lesions. Possibly due to dirt under fingernails. If you itch, you will scratch, if scratch for years then it’s not at all unlikely you would scratch some dirt into your skin.
We then get to “differential diagnosis”, where they purport to show that “Morgellons” cannot be Delusional Parasitosis (DP), Drug induced formication, Scabies, tropical dermatoses (Harvey’s theory) or perforating dermatoses. These arguments seem to be neat little tautologies, which I’ll summarize for flavor:
- Morgellons cannot be DP because the patients were not delusional before they got Morgellons.
- Morgellons cannot be drug induced formication, because the patients don’t take drugs.
- Morgellons cannot be tropical dermatoses, because the patient has not been to the tropics.
- Morgellons cannot be perforating dermatoses because the patients don’t have the genes or the symptoms
The reasoning here is either irrelevant or wrong. Nobody is making any claim that “Morgellons is X”, so demonstrating that “Morgellons” is not filarial worms does not make any real statement about the population of people who have self-diagnosed with Morgellons. Since the most likely explanation for “Morgellons” is that it is a random mixture of physical and mental conditions, varying by individual, that the sufferer’s have self-diagnosed as Morgellons, then you will ALWAYS be able to find many in that group about whom you can say “they do not have X, so Morgellons is not X”. Contrariwise, you can always find some who actually DO have X, but this also does not mean that “Morgellons is X”, it just means X explains the symptoms for that particular patient.
Take “Drug-induced formication”. Some people who think they have Morgellons actually DO have drug-induced formication. It’s not clear how many, but that’s a bit a of straw man, because formication is a symptom of a HUGE range of conditions, including menopause. Of course Savely and Stricker could say “Morgellons is not Menopause, because some of the patients are men”. But that’s just as disingenuous as their other differentials. Some people who have self-diagnosed with Morgellons MUST have menopause-related formication. It’s a statistical certainty. And given that there are around a million regular meth users in the US, it’s almost certain that some of them have drug-induced formication. If you take into account the users of Ritalin, Adderall and Lunesta (all of which have formication as a side effect), then the proportion is much higher.
Then saying that Morgellons is not onchocerciasis because “tropical travel and eosinophilia are not commonly reported in Morgellons patients” is almost funny. Funny because it’s quite true. Funny because it’s the theory that the MRF are about to promote. And funny because it’s the kind of reasoning that Stricker derided the CDC and the IDSA for when they say it’s unlikely that you have Lyme disease if you don’t live in a region where it is endemic, or if your tests come back negative.
It is unfortunate that this paper will be taken seriously when it really boils down to “We don’t know what these people have, but we think that large quantities of antibiotics help some, and doctors should be more open minded.” The publication of this paper will only perpetuate the misunderstandings regarding Morgellons and further drive vulnerable patients into the clutches of quacks and charlatans.