The problem of Morgellons is primarily one of a stark divide between the perceptions of the doctor on one hand, and the patient on the other.
The doctor sees a varied set of physical and mental symptoms that could be caused by one or more conditions. They see lesions on the patient’s body that often look like the patient has scratched themselves. They also see the patient pointing out things on their body, like lint, hair and specks of dirt, and they hear the patient say these things emerged from their body. They hear the patient insist they have a disease called “Morgellons” that has only recently been discovered.
The patient sees the doctor trying to “explain away” what are, to them, obvious symptoms. The patient thinks they feel the the fibers move, and emerge from their body. The patient is frustrated by the doctor’s suggestion that there might be an emotional component to their symptoms. The patient rejects the doctor’s diagnoses and substitutes their own.
In this post, I’m going to focus on the doctor’s perception of these patients. I feel what these fifteen doctors and professors say here really encapsulates and explains many of the problems, and answers many of the arguments surrounding “Morgellons”.
http://www.timesonline.co.uk/article/0,,18393-2188371.html
“This is not a mysterious disease,” says Dr Norman Levine, a Professor of Dermatology at the University of Arizona. “If you polled 10,000 dermatologists, everyone would agree with me.” He says he has seen 100 patients suffering from such symptoms, and they responded well to treatment, including a drug called Pimozide, which is used for chronic schizophrenia. According to Dr Levine, they are suffering from a monosymptomatic disorder in which they are absolutely convinced something is in their skin, a delusional parasitosis. He says he has studied the fibres his patients bring in by the bag-load and they are textile in nature.
http://www.livescience.com/humanbiology/060526_morgellons.html
Michael Girardi, a dermatologist at the Yale School of Medicine, had never heard of Morgellons but when its symptoms were described to him, he was reminded of another disorder that is well known to doctors. “They just renamed it,” Girardi told LiveScience. “We just call it delusions of parasitosis.”
“It’s basically when a patient thinks that there’s something coming out of their skin, a material or bug of some sort, when truthfully there’s nothing there,” said Stacy Beaty, a dermatologist at the Saint Louis University School of Medicine.
In medical schools, physicians learn to watch out for the “matchbox sign” of delusional parasitosis, when patients bring in hair, skin or clothing lint, sometimes in matchboxes, that they claim contain the insects or parasites responsible for their torment. However, when examined, the samples reveal no such thing. The lesions and scratches sometimes seen on patients with delusional parasitosis are usually self-inflicted, Beaty said.
“To rule out any infectious causes and also to put the patient’s mind at ease, a lot of times we’ll do skin biopsies,” Beaty said in a telephone interview. “If we feel that it’ll be helpful, we might also start different anti-psychotic or anti-anxiety medicines.”
In response to rising media coverage about the condition, the Los Angeles Department of Health Services recently issued a statement that said bluntly: “No credible medical or public health association has verified the existence or diagnosis of ‘Morgellons Disease.’ The current description of the disease is vague and covers many conditions.”
http://www.rgj.com/news/stories/html/2004/05/08/70309.php
“In many cases, (delusional parasitosis) is a mono-delusional problem,” Lynch [Dr. Peter Lynch, professor emeritus in dermatology at the University of California, Davis] said. “The patients are normal in every other way. It’s always hard to get such patients to believe it’s a psychological problem. Some patients are very convincing, and I’ve had psychiatrists call me about referrals I’ve made and ask if I’m absolutely sure there’s nothing organic going on here.”
He said in the 40 years he has been practicing medicine he hasn’t seen a delusional parasitosis patient with physical symptoms that can’t be explained. He said while it’s possible some cases may be wrongly diagnosed, it’s unlikely a large segment of patients is suffering from a physical illness.
“You can miss a case and of course that happens,” Lynch said. “But are many being missed? In a word, no.”
http://www.rgj.com/news/stories/html/2004/05/08/70307.php
When told of Dr. Bill Harvey’s successful treatment with antibiotics of Morgellons’ patients in Houston, Dr. Peter Lynch of the University of California, Davis said the “cures” are easily explained by the placebo effect. Patients treated with sugar pills, for example, often get well because they believe they are receiving medicine
Lynch said 80 percent of patients with delusions of parasites respond to psychotropic medication, an indication their illness is mental.
“Anecdotal evidence doesn’t carry much weight,” Lynch said. “There are many anecdotes of alien abductions, but that doesn’t mean they are true. And as for the pictures, you can see pictures of the Loch Ness Monster on the Internet, too.”
“If there were a peer-reviewed study, with 15 or 20 patients who have the same exact thing in their skins, then maybe I’d believe it,” Lynch said. “When fiberglass curtains first came out, many people with skin conditions were diagnosed with delusions of parasitosis (DOP). But studies showed these patients had tiny (fiberglass particles) in their skin.”
http://www.sfgate.com/cgi-bin/article.cgi?f=/c/a/2006/06/02/MNGOJJ6JO51.DTL&hw=Morgellons&sn=001&sc=1000
“There are a huge number of people out there with (delusional parasitosis), and most of them are not getting adequate treatment because they have this fixed belief,” said Dr. Dan Eisen, a UC Davis dermatologist. “It’s probably just a group of patients who haven’t gotten the appropriate treatment, and they’re calling it Morgellons.”
http://www.popularmechanics.com/science/medicine/1662162.html
“Dermatologists are afraid to see these patients,” says Dr. Peter Lynch, professor emeritus of dermatology at the University of California, Davis. He says he has examined about 75 people with Morgellons-like symptoms in the past 35 years and believes they suffer from delusional parasitosis–literally, delusions of parasites in the skin. It’s a diagnosis people don’t like. One patient, threatening malpractice, convinced the state medical board to investigate Lynch. Another warned he had a pistol in the glove compartment of his truck, Lynch says. “He told me, ‘I’m going to shoot the next doctor who tells me it’s in my head.'”
Another prominent dermatologist, who insisted on anonymity out of concern for his safety, says he has diagnosed 50 or so Morgellons patients with cutaneous dysaesthesia–a neurological disorder that can result in the sensation of scuttling insects. And the spiny things? “In every case I’ve seen it’s a textile fiber, and it’s on the surface of the skin,” he says. He typically puts a cast over the lesions to prevent further irritation and after four weeks removes it. “Guess what?” he says. “The lesions are healed.”
http://www.dallasobserver.com/Issues/2006-07-20/news/feature_full.html
Part of the problem with a disease like Morgellons, [Tim Jones, an epidemiologist from the Tennessee Department of Health] says, is that its symptoms are both vague and varied. Before public health officials can investigate, there must be a clear definition of the disease. The Morgellons Research Foundation says they have that definition, but there is no one symptom, or even group of symptoms, that defines Morgellons. […]
“Trying to do studies on a group like this becomes virtually impossible because you may have 10 percent of the people who meet a real strict definition and a whole bunch of other people who don’t,” Jones says. “If you go through 10 patients and one is having discolored sweat, another one’s having pieces of spaghetti stick out of his skin and another one’s having, I don’t know, heel pain, it’s really hard to think what would tie these things together”.
http://www.post-gazette.com/pg/06204/707970-85.stm
“They suffer terribly, but it’s psychiatric,” said Dr. Dirk Elston, a dermatologist in the Geisinger Medical System in Danville, Montour County. “The fact that there’s something online to cling to, it’s a difficult obstacle for us.”
“The moment you mention psychiatrists, these patients get extremely angry,” said psychiatrist Alistair Munro, author of “Delusional Disorder.” “They say there’s nothing wrong with their brain. They have all kinds of explanations.”
“I found no evidence of [anything suspicious] in Andrew,” Dr. Heldrich [Dr. Fred Heldrich, a Johns Hopkins pediatrician] wrote to Dr. Frac after the visit. Then he added: “Ms. Leitao would benefit from a psychiatric evaluation and support, whether Andrew has Morgellons disease or not. I hope she will cease to use her son in further exploring this problem.”
http://home.hamptonroads.com/stories/story.cfm?story=110940&ran=130308
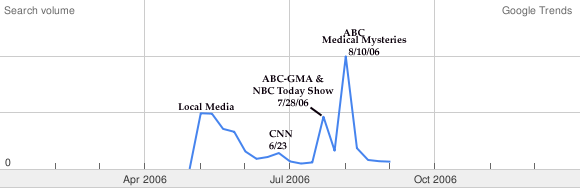
“People don’t need the Internet as long as they’ve got the media,” said Edward Shorter, a professor of psychiatry and the history of medicine at the University of Toronto. Once the media reports come out about a new possible disease, even if it’s not real, some people see it, “and they say, ‘That’s what I’ve got. That’s my disease,'”
http://www.click2houston.com/health/4246515/detail.html
“I always feel that people should keep an open mind and I think there are scientific experiments, what we call evidence-based medicine, that can prove or disprove that an organism is causing this,” University of Texas Health Science Center at Houston dermatologist Dr. Stephen Tucker said.
http://seattletimes.nwsource.com/html/nationworld/2003152087_illness26.html
“In dermatology, we speak about something called an ‘outside job,’ which is a skin eruption made by the patient himself,” said Dr. Noah Scheinfeld, an assistant professor of dermatology at Columbia University in New York and an expert on the psychiatric origins of certain skin disorders. “When you look at the pictures of these Morgellons lesions, they are classic for that.”
http://www.ent.uga.edu/publications/delusory.pdf
Self-excoriation is a common feature of delusory parasitosis, despite the individuals’ protestations that they do not scratch. Scratching may produce papular eruptions. Any repeated skin irritation produces a friction blister. Repeated rubbing of an area often produces a bleb (small blister) which, when ruptured, yields an open sore that may become infected. Once the sore begins oozing plasma and a scab forms, hairs and cloth fibers become entrapped in the sticky fluid. These flecks are dislodged and called mites or insects because they look like they have “antennae” and “legs”. Hair follicles often are pulled out; the follicle accompanied by the associated sebaceous gland looks like a worm. – Nancy C.Hinkle, Professor of Entomology, University of Georgia.
http://www.emedicine.com/derm/topic941.htm
Patients pick at areas until they can pull material from the skin. This may be referred to as “pulling a thread from the skin.” – Dr. Noah Scheinfeld,
http://www.rangelmd.com/2006/08/there-are-these-little-fibers-coming.htm
Logically, any credible study of Morgellons should have tried to explain the connection between the fibers and the symptoms. It’s not a good sign that no one has bothered to offer a formal starting theory on Morgellons fibers and that the [Morgellons Research] Foundation criticizes physicians for not looking for signs of Morgellons when they don’t really know what to look for themselves. – Dr. Chris Rangel, MD.
http://www.nature.com/news/2006/060828/full/nm0906-982a.html
Noah Scheinfeld, assistant clinical professor of dermatology at Columbia University, says patients sometimes come in with pieces of their skin mixed with other materials in a box or a piece of Saran Wrap. “Such patients are a challenge to help and to treat,” he says. “They want to be believed above all and tend to be socially isolated.” Scheinfeld says the Internet has helped those with parasitic delusions to band together and reinforce each others’ beliefs.
“There really is no scientific basis at this point to believe that [Morgellons] is real,” says Stephen Stone, president of the American Academy of Dermatology.