The CDC today released a “Request for Quotations” for their Morgellons investigation, which is basically a formality, as the only entity they would qualify to do the work is Kaiser. They also listed the lab tests that would be done (basically all the standard systemic tests).
http://www.fbo.gov/spg/HHS/CDCP/PGOA/Reference%2DNumber%2D2007%2DMorgellons/Attachments.html
They give a list of the work to be done:
2.1. Describe the clinical and epidemiologic features of persons who have reported themselves as having this unexplained skin condition, including assessing the frequency of co-morbid conditions (e.g., neurocognitive deficits, neurologic conditions, major psychiatric disorders).
2.2. Collect information to generate hypotheses about possible risk factors for this condition.
2.3. Assess the histopathologic features of the skin condition based on skin biopsies from a sample of affected patients.
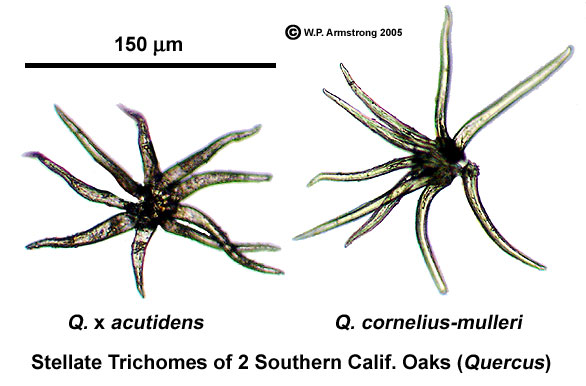
2.4. Characterize fibers or threads obtained from patients with the condition to determine their potential etiology.
2.5. Describe the geographic distribution and estimate rates of illness.
2.6. Describe health care utilization among persons with the condition.
And a timeline:
4.1. IRB [Independent Review Board] Clearance October 30, 2007
4.2. Database of potential cases (study cohort) November 30, 2007
4.3. Database containing all results of clinical evaluations, Including recorded histories and physicals, laboratory tests (See Attachment 001 for required laboratory tests), chest x-rays, digital photos, neuorcognitive/neuropsychiatric examinations. March 1, 2008
4.4. All skin biopsy specimens and fiber samples collected from case-patients . March 1, 2008
4.5. Electronic database containing demographic information, zip code of residence, relevant past health history, such as medications, provider visits, and hospitalizations for cases. Database should include a unique patient identifier to allow linkage of clinical and other test results with demographic, healthcare utilization, and survey data. April 30, 2008
4.6. Database with denominators for all visits (total and by specialty) and hospitalizations during study period to allow estimation of disease rates in the population. May 30, 2008
That’s exactly what you should do if there is some evidence of a new infectious disease, parasite or environmental contamination. You get a patient population (the “study cohort”), and you investigate their symptoms, and see what they have in common, and look for common risk factors and diagnostic markers that might indicate a cause.
What’s a bit unusual here is that the patient population is “persons who have reported themselves as having this unexplained skin condition”, in other words: “people who think they have Morgellons”. This entire study is simply of people who THINK they have Morgellons. Very interesting.
The CDC are investigating Morgellons because it is an “emerging public health problem” and they have “received an increased number of inquiries from the public, health care providers, public health officials, Congress, and the media“, and “some who suffer from this condition appear to have substantial morbidity and social dysfunction, which can include decreased work productivity or job loss, total disability, familial estrangement, divorce, loss of child custody, home abandonment, and suicidal ideation“. All true, but with contested causation.
But wait a moment, why is the CDC getting ready to spend millions of dollars investigating Morgellons, when they simply could go to Oklahoma State University, where:
http://www.healthsciences.okstate.edu/morgellons/vision.cfm
OSU-CHS physicians/researchers have physical evidence of Morgellons Disease
– Morgellons is not psychiatric in origin
– Morgellons is an emergent disease
No only that, but they already have a patient population all of which can be instantly diagnosed by the appearance of fibers under the skin.
http://www.healthsciences.okstate.edu/morgellons/docs/Wymore-position-statement-2-19-07.pdf
Of the thirty or so patients claiming to have Morgellons disease, that clinical faculty have examined in facilities associated with OSU, only one patient likely did not have Morgellons.
…
100% of the patients, that were felt to genuinely have Morgellons Disease, have large microscopic-to small macroscopic fibers visible under their outer layer of skin.
There are doctors and professors there who have been looking at this for years, and have sufficient evidence to convince themselves 100%:
http://www.mysanantonio.com/news/medical/stories/MYSA072406.morgellons.KENS.1e13fade.html
“I am 100 percent convinced that Morgellons is a real disease pathology,” said Dr. Randy Wymore, an assistant professor of pharmacology and physiology at OSU.
…
Dr. Rhonda Casey has examined more than 30 Morgellons patients.
“There’s no question in my mind that it’s a real disease,” she said.
So if Oklahoma State University has already figured this out, why don’t they help out the CDC? Do they actually have any evidence? Could it be they’ve been a little hasty in their certainty? Perhaps a little unscientific? Or could they save the CDC some money?


 Why does the Morgellons idea persist, when there is no evidence to support it?
Why does the Morgellons idea persist, when there is no evidence to support it?