On the Morgellons research foundation, there is a flashing link that says “Click here for a letter to your doctor!”, which takes you to this page:
http://www.morgellons.org/letter.pdf
This is a two page letter, with the Oklahoma State University CHS letterhead, dated May 15, 2006, from Randy S. Wymore, Ph.D. and Rhonda Casey, D.O., beginning “Dear Practicioner,”
The letter makes some interesting claims, and contains a few leaps in reasoning, and unspoken assumptions. I’ll go over the whole letter and comment on it a bit at a time.
This letter concerns a patient population that manifests a particular set of symptoms we have encountered with increasing frequency, and that OSU-CHS is actively researching. The condition has been labeled as Morgellons Disease and it is unclear if this is a single disease or a multi-faceted syndrome.
What is unclear is if there actually is a patient population manifesting a particular set of symptoms. As has been pointed out several times, including by the Los Angeles Department of health, the “particular set of symptoms” is vague and covers a large number of conditions. The only consistent distinguishing feature, the fibers, has been shown to be simple environment contamination, since fibers are everywhere and it is impossible to keep them out of lesions.
Until recently, most of these patients have been grouped as a subset of the diagnosis of Delusions of Parasites (delusional parasitosis; DOP).
Delusions of Parasites is the mistaken belief that one is infested with parasites. If people simply have lesions, and find fibers in them, they may form the mistaken belief that their fibers are connected with their disease. DOP is a poor diagnosis in this case, and I have often spoken against this.
The Morgellons research foundation seek to characterise their campaign as a fight between two choices, either Morgellons is a new disease, or it is DOP. This serves to increase sympathy for sufferer, as clearly their symptoms (particularly the lesions) are real, and they do in fact find fibers in their lesions. But the reality is more complex. Many of the sufferers clearly have some form of dermatitis artefacta, or neurotic ecoriations, and the causes of those symptoms are many and varied, and DOP plays only a small part in them.
After obtaining careful patient histories and thorough physical exam, we have determined that Morgellons patients have several important distinctions ruling out the diagnosis of DOP.
Like I said, DOP plays only a small part here. So ruling it out only rules out a small part of the possible causes of the symptoms. There are a LOT of other things that need to be ruled out before we can decide someone has a disease new to science.
This population of patients frequently exhibit the following symptoms:
• Distinct and poorly healing skin lesions with unusually thick, membranous scarring upon eventual healing.
A classic sign of Neurotic Excoriations. Dr Noah Sheinfeld, MD, JD, FAAD, says of Neurotic Excoriations: “The erosions and scars of NEs often have irregular borders and are usually similar in size and shape”, “The erosions can heal slowly because of recurrent picking”, “Scars often remain on patients with this condition”, “Patients pick at areas until they can pull material from the skin. This may be referred to as ‘pulling a thread from the skin.’”
• Moderate to extreme pruritis at sites of lesions as well as un-erupted skin.
Pruritis (itching) has many causes. That lesions should itch is not at all surprising. Itching can cause lesions via what is known as the itch-scratch-itch cycle, whereby the patient obtains temporary relief via scratching, but irritates and damages the skin in the process, causing the itching to return later. Eventually the damage to the skin causes lesions to form. The Merk manual says “chronic rubbing or picking at itchy skin results in an “itch-scratch-itch ” cycle that can eventually progress to discolored thickened patches of skin (lichen simplex chronicus) and/or lumps and swellings (prurigo nodularis) that are difficult to treat” – note that “lichen simplex chronicus” sounds similar to the “unusually thick, membranous scarring” that is mentioned above.
• Microscopic examination of these lesions will most often reveal the presence of unusual fibers, which may be black, blue or red. These fibers, which many healthcare providers initially thought to be textile contaminants, are often present in the deep tissue of biopsies obtained from unbroken skin of individuals with this condition. Careful examination of these fibers further reveals that they are frequently associated with hair follicles, and are definitely not textile in origin.
I’ve covered fibers before, demonstrating that fibers are everwhere, and that I personally have fibers on my skin, and in my lesions. I’ve not performed a deep tissue biopsy yet, but I wonder how many Wymore and Casey have performed, and if they did, were the results anything like this:
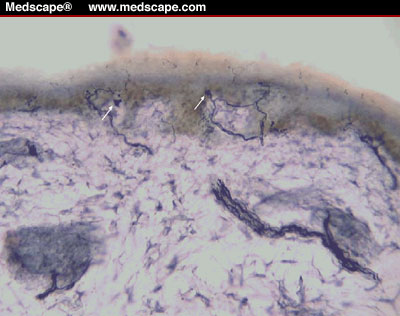
That’s a deep skin biopsy clearly showing some fibers. They are nerve fibers.
But what of “not textile in origin”? It is unclear how this has been determined, how many fibers have been examined, and what the source of those fibers was. Wymore has simply failed to identify some fibers out of the hundreds he has looked at. He is not an expert on fiber analysis, and even the experts can not identify every fiber they look at. Not being able to identify a fiber tells you nothing.
“Black, red and blue“? Along with clear and white fibers, which are hard to see on skin, those colors are by far the most common in environmental fibers, accounting for seemingly over 95% of all random fibers I have observed.
• Most of these patients suffer from a host of neurological symptoms which can vary in severity from mild to severe. These neurological symptoms include peripheral tingling, paresthesias and varying degrees of motor involvement which appear to progress.
That describes just about everyone over the age of 40. If you were to ask any patient of middle age or above: “have you ever felt any numbness, or tingling”, you’d probably get an affirmative answer. The cause could be anything from very common conditions such as Carpel Tunnel Syndrome, arthritis, diabetes, hypothyroidism or atherosclerosis, to less common, but not unusual, conditions such as a brain tumor, motor neurone disease, or autoimmune disorders like multiple sclerosis or lupus erythematosus.
• Intermittent cognitive and behavioral status changes are often observed and also seem to progress with the severity of disease. This is often referred to as “brain fog” by the patient as they experience a waxing and waning of this symptom.
“Brain fog” is common symptom of Chronic Fatigue Syndrome, a MUPS that many Morgellons believers are diagnosed with. “Intermittent cognitive and behavioral status changes” can have many causes, including normal aging.
• Laboratory findings in these patients are variable, but often reveal eosinophilia and elevated levels of Immunoglobin E.
“Eosinophilia” is a blood test result indicating an increase in the amount of eosinophils in the blood. A “wide spectrum of illness” is associated with this. The most common cause in the US is “allergic conditions, including drug reactions and atopic asthma”. Worldwide it can be an indication of parasitic infection, which explains its popularity with some Morgellons believers, who often claim their doctors are too quick to discount exotic illnesses such as parasitic worms.
“Immunoglobulin E” (IgE) is a type of antibody. Some people have elevated levels of IgE, which seems to be related to a higher incidence of allergies, eczema and asthma. One can see some correlation here with conditions that have symptoms that might lead people to believe they have Morgellons.
There is another simple explanation for elevated IgE levels, Dr. Adrezej Szczeklik notes “Tissue injury characteristically results in a marked, transient rise in IgE levels in the blood“. While this is more typically associated with major trauma, it’s quite conceivable that the the same mechanisms come into play when the body is dealing with the persistent healing situation presented by the continually generated lesions, and likely sepsis, of neurotic excoriations.
• Other symptoms of varying severity and frequency have been described, and are included in the attached case definition.
As I’ve discussed before, the case definition is all-encompassing. I fit well within the case definition, yet I don’t have Morgellons.
Morgellons patients differ from classical, delusional parasitosis patients in several areas. They do not respond to antipsychotics,
If they simply had eczema with itching (a perfectly normal condition), and found some fibers on their skin, then antipychotics would not help. Again though, this is not DOP vs. Morgellons. A vast number of conditions could cause these symptoms, many of which would not respond to antipsychotics. Also, this is based on what evidence? Clinical studies, or anecdotes?
and new lesions continue to appear upon complete cessation of manual excoriation.
Again, what is the evidence? I suspect this is based on anecdotal self-reporting by the patients. Actual dermatologists suggest otherwise: “He typically puts a cast over the lesions to prevent further irritation and after four weeks removes it. ‘Guess what?’ he says. ‘The lesions are healed.’”
Due to the sensation of foreign material in their tissue, that has been described as sharp, stinging and/or splinterlike, the patient may have discovered the fibers prior to seeking medical care, and may bring them to your office for examination. Please do not assume that the patient’s problem is purely psychological based on this propensity.
What is being referred to here is the “matchbox sign“. The patient itches, the patient thinks this feels like a splinter, they look at their skin, they see fibers, they assume they are related to the itching, they take them to the doctors. Doctors will not assume these patients are delusional – they will explain that the fibers are lint, they might examine them to verify this. They will only begin to consider a delusional disorder if the patient continues to insist that the fibers are somehow unusual, in the face of contrary evidence. Further diagnosis of DOP may come if the patient insists that the fibers are some kind of organism, based on no evidence.
The “Matchbox sign” alone is not an indication of a psychological disorder. Nancy Hinkle lists twenty common attributes of DOP sufferers, of which the matchbox sign is just one. However, since it IS a symptom of DOP, the physician must take this possibility into account.
Many of these patients may appear skeptical of traditional medical care due to frequent dismissal of their symptoms in the past. The combination of suffering from a chronic disease with distressful symptoms and no known cause or cure can cause some patients to appear anxious or agitated. We encourage you to take the time to carefully interview any patient who may fall into this category, perform any testing you may deem appropriate, and most importantly treat the patient with compassion and dignity.
This last part I fully agree with. These are real people with real problems, they deserve our sympathy, our compassion, and the best medical efforts to help them recover from whatever is causing their symptoms.







{kind=link}
{kind=link}